
A vitelliform-like lesion and the pattern that gives it away
A 77-year-old woman was referred by her optometrist after noticing a change in her colour vision and a reduction in near vision. OCT showed a vitelliform-like lesion close to the left fovea that had not been present on a scan taken two months earlier. Visual acuity was 6/9 bilaterally with N6 near vision. She was initially seen in the emergency eye department where no acute pathology was identified, and was subsequently reviewed in the medical retina clinic.
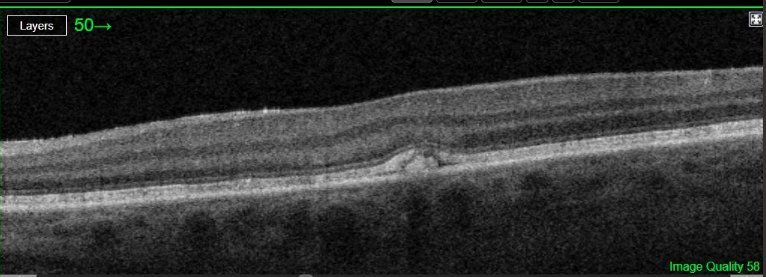
Macular OCT - left eye, submitted with the original referral. A subtle hyperreflective deposit at the level of the RPE with mild outer retinal disruption, producing a vitelliform-like appearance that prompted the referral.
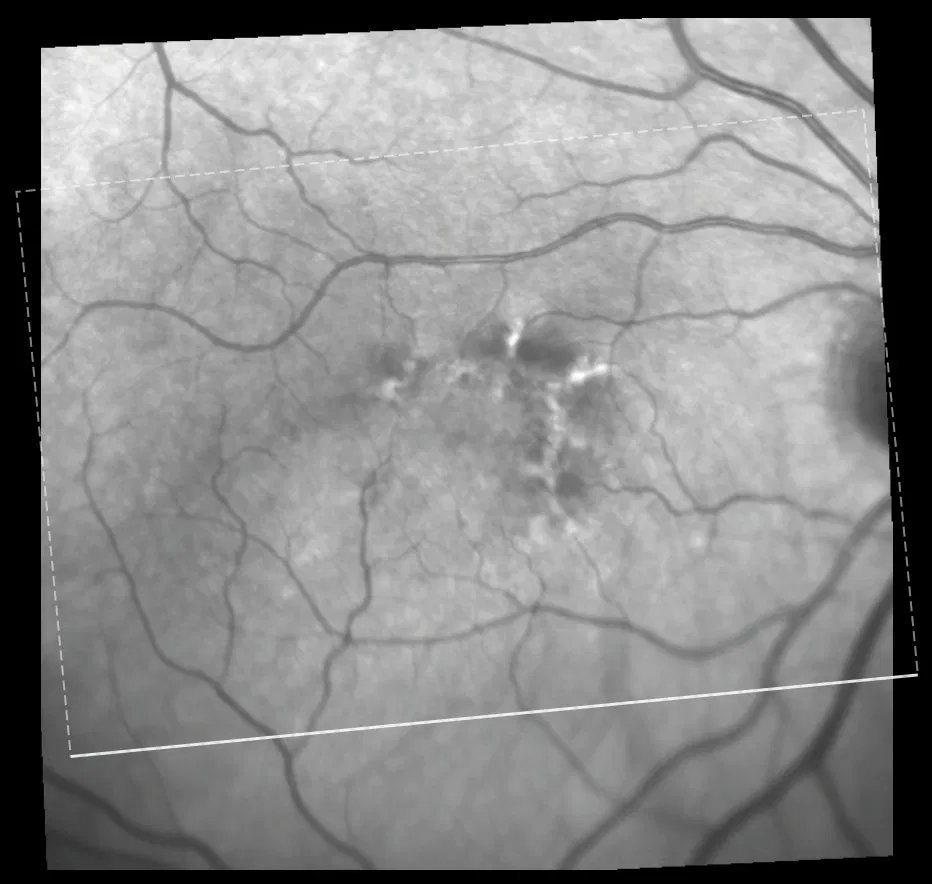
Near-infrared fundus image - right eye. Characteristic macular pigment changes in a cruciform distribution at the level of the RPE, consistent with butterfly-shaped pattern dystrophy.
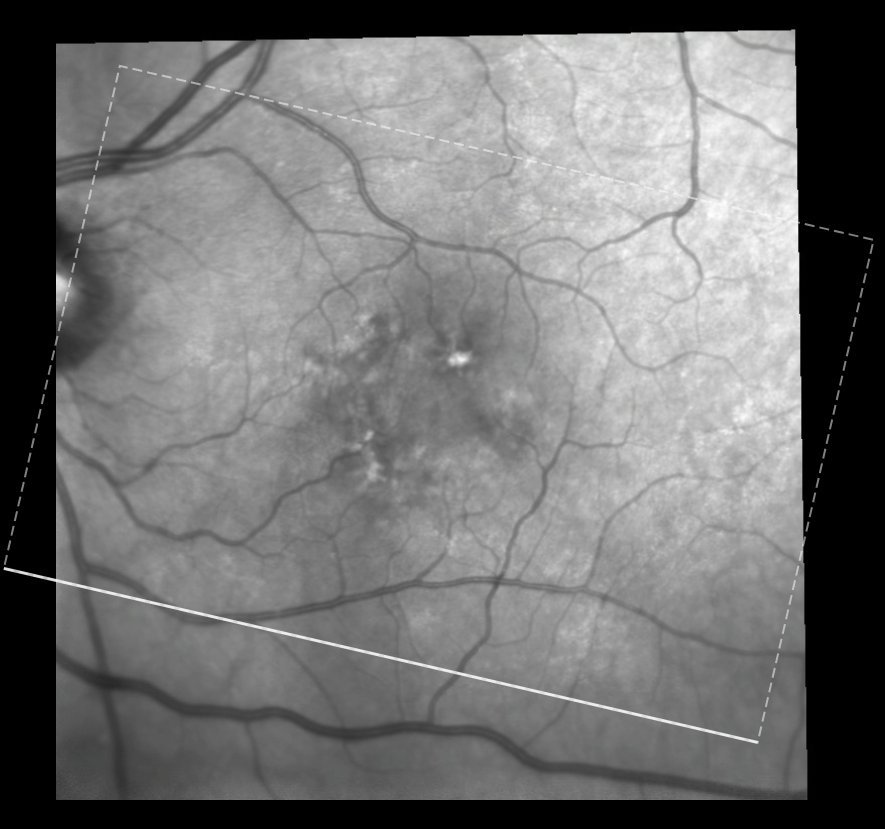
Near-infrared fundus image - left eye. Similar cruciform pigmentary changes, slightly more pronounced than the right.
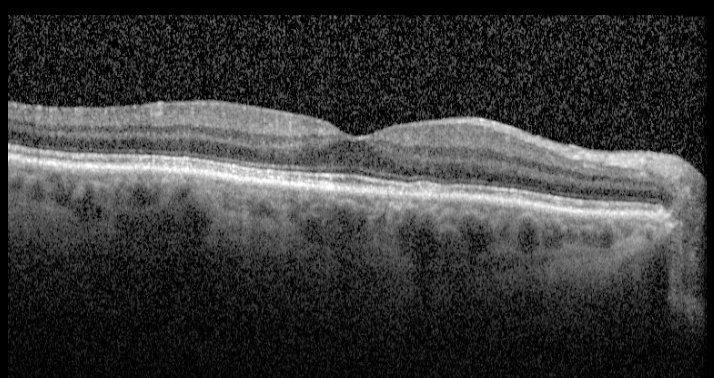
Macular OCT - right eye. Hyperreflective deposits at the RPE level with mild outer retinal disruption. No subretinal fluid.
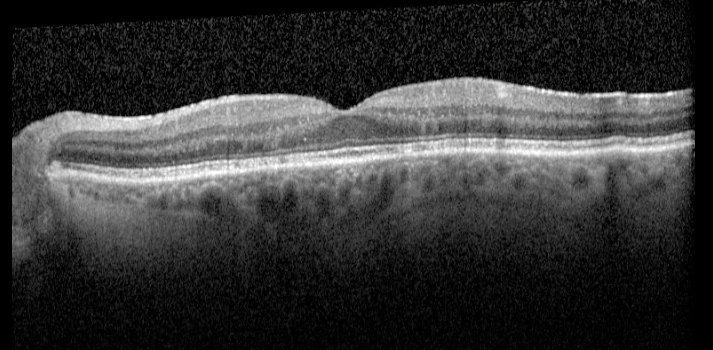
Macular OCT - left eye. More prominent hyperreflective deposits at the RPE level producing a vitelliform-like appearance. No subretinal fluid.
The near-infrared fundus images are the key to diagnosis here. Both eyes show a cruciform or butterfly distribution of pigment changes at the level of the RPE - a pattern that is immediately recognisable as butterfly-shaped pattern dystrophy , one of the pattern dystrophies of the macula, a group of slowly progressive autosomal dominant conditions characterised by abnormal lipofuscin deposition at the RPE. The OCT findings of hyperreflective RPE-level deposits with a vitelliform-like appearance in the left eye are well recognised in pattern dystrophy and do not represent a true vitelliform lesion. Crucially, there are no drusen - an absence that steers the diagnosis away from AMD, with which pattern dystrophy is frequently confused in older patients.
The optometrist noted that the left macular change appeared to have developed over two months. Pattern dystrophy does not evolve on this timescale - it is likely that a subtle lesion was present but not detected on the earlier scan. This case is a reminder that the near-infrared fundus image, often overlooked in favour of the OCT B-scan, can provide the decisive diagnostic clue: the bilateral cruciform pattern visible here is not apparent on OCT alone.
This patient will be reviewed at six-monthly intervals with SOS return, moving to annual review if stable. As with early AMD - with which pattern dystrophy shares a similar monitoring approach - patients should be advised to report any sudden change in vision promptly, to monitor each eye separately using an Amsler grid, and to maintain a healthy lifestyle including not smoking. Surveillance is important given the small but recognised risk of secondary choroidal neovascularisation. Further information about macular conditions and monitoring advice can be found in the AMD patient information leaflet on this website.