
Aripiprazole-associated chorioretinopathy with bilateral subretinal fluid
A 43-year-old man with a background of schizophrenia and alcohol misuse was referred with bilateral blurred vision and subretinal fluid on OCT, presumed to represent central serous chorioretinopathy (CSCR) . He had pre-existing left amblyopia. Visual acuity at presentation measured 6/18 right and 6/60 left. He had been referred for consideration of photodynamic therapy (PDT).
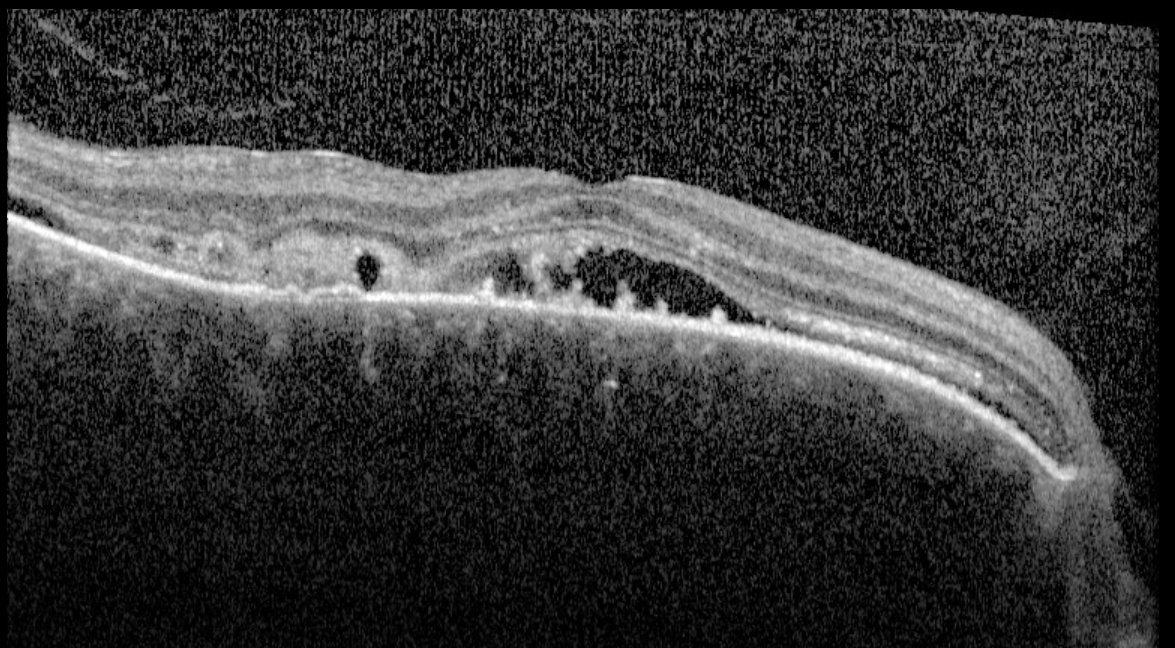
Macular OCT - right eye. Subretinal fluid with hyperreflective subretinal deposits at the RPE surface, consistent with chronicity.
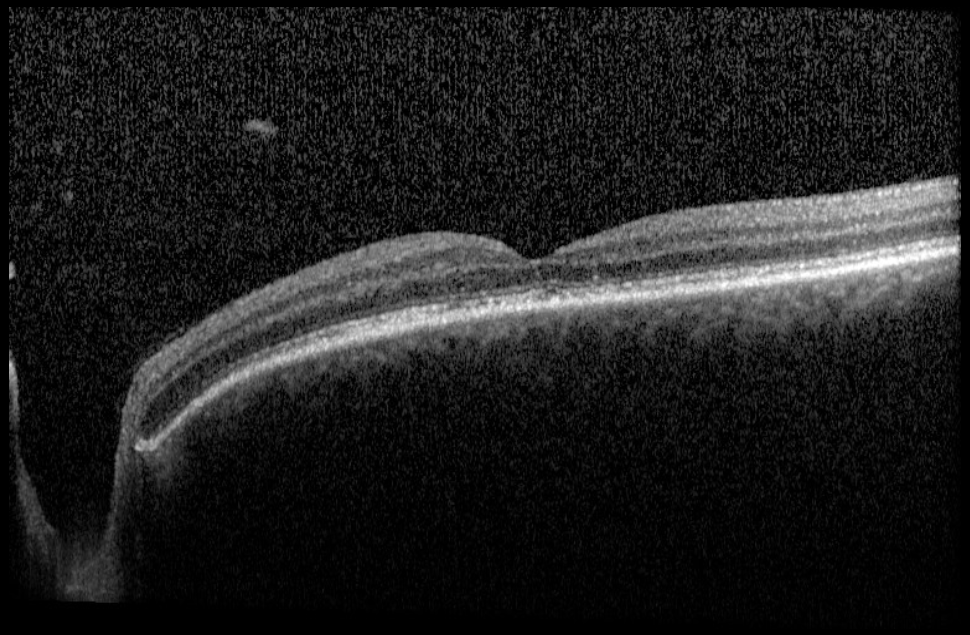
Macular OCT - left eye. Resolution of subretinal fluid. Some RPE disruption.
On review, the left eye showed complete resolution of subretinal fluid. The right eye demonstrated stable subretinal fluid with subretinal hyperreflective material (SRHM) at the fovea. Detailed drug history identified long-term use of aripiprazole, an atypical antipsychotic with a recognised association with chorioretinopathy.
Aripiprazole-induced chorioretinopathy. Aripiprazole is a partial dopamine D2 agonist and serotonin 5-HT2A antagonist. Both dopamine and serotonin pathways are implicated in the regulation of choroidal vascular permeability, and disruption of these systems is thought to underlie drug-associated CSCR-like presentations - a mechanism described in the context of related atypical antipsychotics such as quetiapine . The first published case of aripiprazole-induced chorioretinopathy was reported by Moschos et al. (2015) , describing a patient with schizophrenia on long-term aripiprazole who developed serous retinal detachment and outer retinal atrophy on multimodal imaging. In the current case, spontaneous resolution of the left SRF - without any change in treatment - is consistent with the fluctuating natural history seen in drug-associated CSCR.
The obvious intervention would be withdrawal of aripiprazole. However, this patient is subject to a conditional discharge from secure psychiatric care, with continued antipsychotic treatment a condition of that licence. Liaison with his responsible psychiatrist confirmed that the risk of psychotic relapse - and the serious consequences that would carry for the patient and others - outweighed the immediate threat to vision. Aripiprazole was therefore continued. The patient was counselled at length about the nature of the association and the competing risks involved in this decision.
He will proceed to FFA and ICG angiography. Should angiography confirm an active leakage point amenable to treatment, PDT will be considered using the same criteria applied to idiopathic CSCR. Ongoing ophthalmological review will be maintained in close liaison with his psychiatric team. This case illustrates the importance of drug history in CSCR, especially in bilateral cases, and that management decisions may extend well beyond the retina clinic.