
Peripapillary choroidal neovascular membrane detected on routine sight test
An 83-year-old woman was referred following a routine sight test at which she had no visual symptoms and stable refraction. Visual acuity measured 6/15 right and 6/12 left, correcting to 6/6 bilaterally. Intraocular pressures were 12 mmHg right and 11 mmHg left. The optometrist noted a peripapillary haemorrhage on left fundus photography and performed an OCT, identifying thickening near the photoreceptor layer with possible intraretinal fluid. A right OCT was not submitted with the referral, but was presumed normal given the absence of any concern documented.
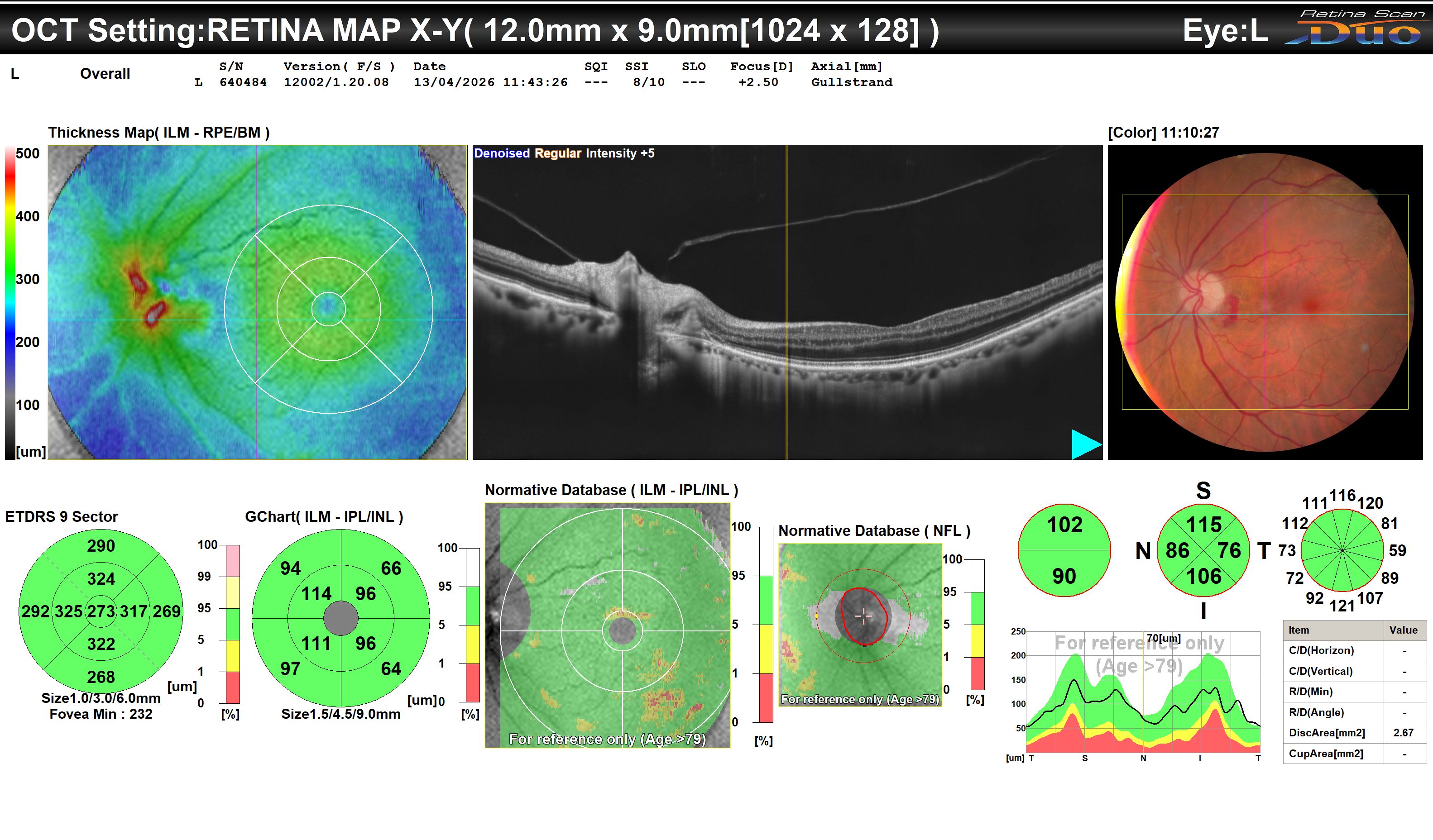
Left eye. Peripapillary haemorrhage temporal to the optic disc on fundus photography. OCT shows a dome-shaped hyperreflective subretinal lesion temporal to the left optic disc with associated subretinal fluid and outer retinal disruption. The fovea is uninvolved. Focal thickening on the thickness map corresponds to the peripapillary lesion.
The left OCT shows a dome-shaped hyperreflective subretinal lesion temporal to the left optic disc, with a small amount of overlying subretinal fluid and disruption of the outer retinal layers. The fovea is not involved. The fundus photograph confirms peripapillary haemorrhage at the corresponding location. Together, these findings are consistent with an active peripapillary choroidal neovascular membrane (CNVM) .
The main differential in this age group would be polypoidal choroidal vasculopathy (PCV) , but the thin choroid visible on OCT makes this less likely - PCV tends to be associated with pachychoroid. The relative absence of drusen is notable but does not exclude an AMD aetiology; peripapillary CNVM in older patients shares risk factors with neovascular AMD and may occur without typical macular drusen.
This patient will be seen in the macular clinic within four weeks for formal assessment (+/- OCT angiography or fluorescein angiography to characterise the membrane). Given that the fovea is not currently threatened and the natural history of peripapillary CNVM can be self-limited, the initial plan is to observe and to consider treatment only if the membrane extends to threaten central vision. This case is a reminder that peripapillary haemorrhage on fundus photography warrants OCT and prompt referral, even in the absence of symptoms.