
When the age doesn't fit the diagnosis
A 57-year-old man was referred by his optometrist having recently moved to Brighton. He had been under annual macular review at a hospital eye service in east London for approximately 20 years, with a diagnosis of early-onset dry age-related macular degeneration recorded since his late thirties. Best corrected visual acuity was 6/6 right and 6/6 left. He was referred to allow continuity of monitoring locally.
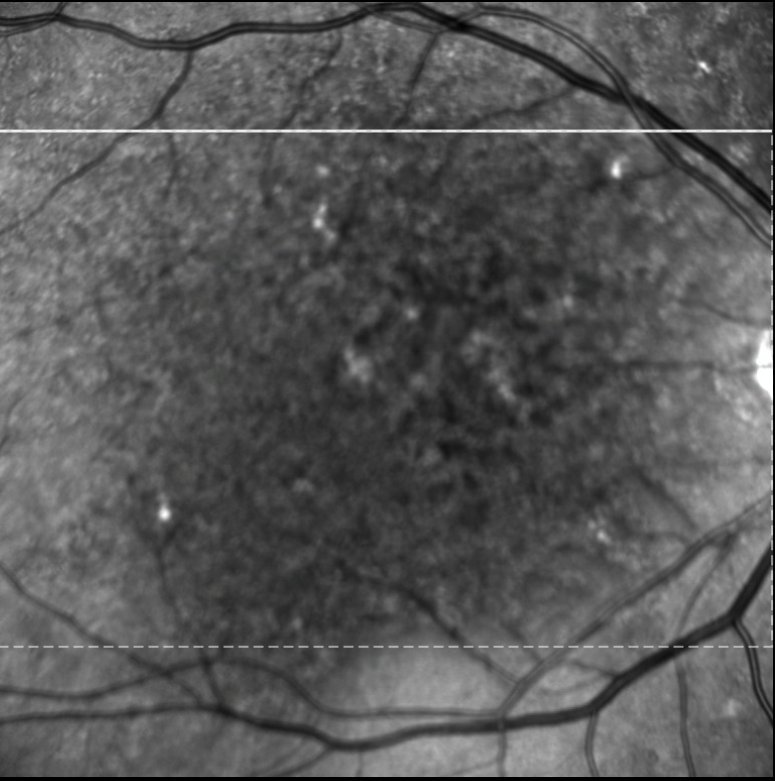
Near-infrared fundus image - right eye. Extensive dark macular area with scattered hyperreflective deposits, indicating widespread RPE and photoreceptor disruption across the posterior pole.
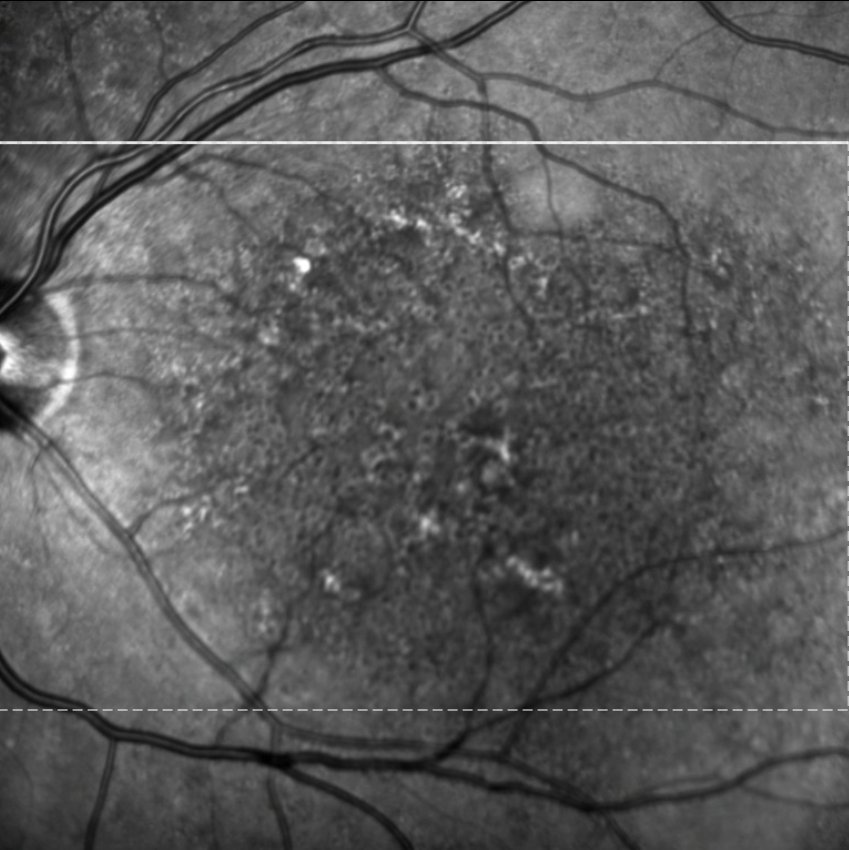
Near-infrared fundus image - left eye. Similar extensive macular changes, with dark irregular atrophy and scattered deposits extending across the posterior pole.
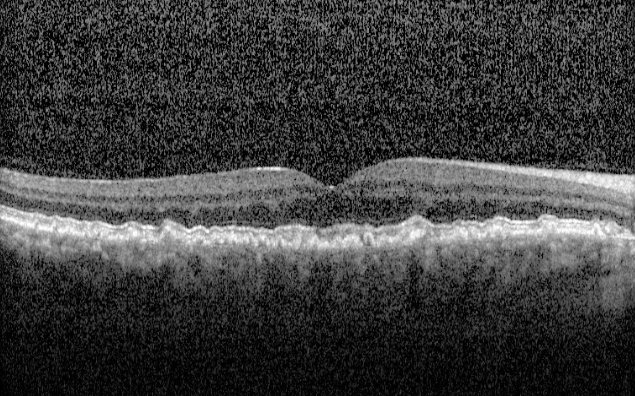
Macular OCT - right eye. Irregular dome-shaped sub-RPE and subretinal deposits with RPE disruption throughout the macular area.
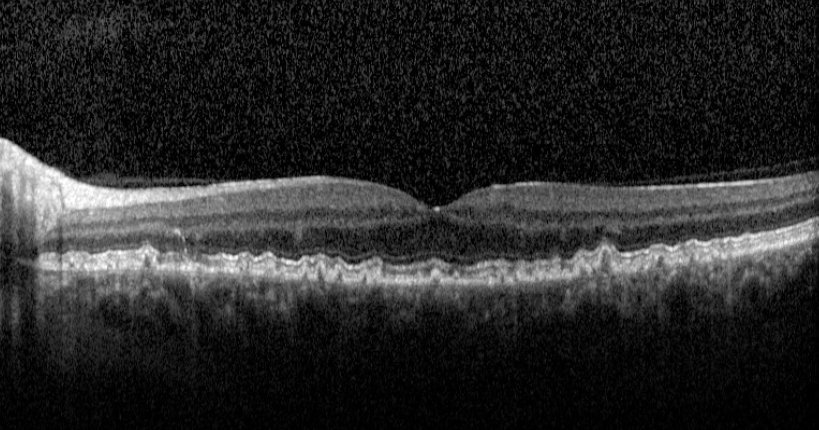
Macular OCT - left eye. Similar lobular subretinal and sub-RPE deposits with widespread RPE irregularity.
The imaging shows bilateral, symmetric macular changes with extensive drusenoid sub-RPE deposits and overlying RPE disruption - findings consistent with a significant inherited macular dystrophy. The AMD label warrants scrutiny. Age-related macular degeneration is, by definition, a disease of older age; onset in the late thirties is not consistent with AMD, though it is worth noting that this patient is now approaching an age at which AMD could plausibly begin to contribute. The most important differential is dominant drusen associated with an EFEMP1 mutation - an autosomal dominant condition that produces early-onset macular and peripapillary drusen in a radial or honeycomb pattern closely mimicking AMD, and known eponymously as Doyne honeycomb retinal dystrophy or malattia leventinese. The relatively thick choroid visible on OCT supports this diagnosis, though it also raises a further consideration: pachychoroid drusen, an increasingly recognised phenotype within the pachychoroid spectrum in which large, sparse drusen occur in association with a thick choroid and dilated outer choroidal vessels, and which some authors have proposed as a discrete inherited condition distinct from AMD. Stargardt disease , the other major inherited macular dystrophy in the differential, is typically associated with a normal or thin choroid and the characteristic “dark choroid” sign on fluorescein angiography, making it an unlikely diagnosis here. Pattern dystrophy is a further consideration. Genetic testing is important in distinguishing between these conditions and has implications for prognosis, family screening, and eligibility for clinical trials.
Correspondence has been sent to Moorfields Eye Hospital, where this patient was originally investigated, to obtain prior imaging, any genetic test results, and the basis for the original diagnosis. This patient will be seen in a medical retina clinic for formal review. As with AMD, patients with inherited macular dystrophies benefit from the same lifestyle and monitoring approach - Amsler grid self-monitoring of each eye separately, prompt reporting of any sudden change in vision, and a healthy lifestyle avoiding smoking. Further information is available in the AMD patient information leaflet on this website.